

Abstract
Background: In the current era, autologous stem cell transplant (ASCT) remains an effective form of treatment for patients diagnosed with multiple myeloma (MM), but it is not curative and a relapse is inevitable. A second, or salvage, ASCT provides better outcomes than conventional chemotherapy but it is infrequently used. Maintenance therapy after initial ASCT has been adopted as the standard in the US; however, there is limited data on the effects of maintenance therapy following salvage ASCT and the benefits are still unclear.
Methods: We performed retrospective chart review of all patients with MM who received a second, salvage ASCT at time of first relapse at Washington University in St. Louis from 2008 to 2016. We identified two cohorts of patients, those who received maintenance therapy following salvage ASCT and those who did not. Patients who received maintenance therapy post-initial ASCT were excluded as the objective of this study was to determine the impact of maintenance post-salvage ASCT and maintenance post-initial ASCT may confound the results.
Results: Sixty-five patients (who underwent second/salvage ASCT) were identified. Three were excluded from the analysis-two had treatment-related mortality following salvage ASCT and one received maintenance other than a proteasome inhibitor (PI) or an immunomodulatory drug (IMID).
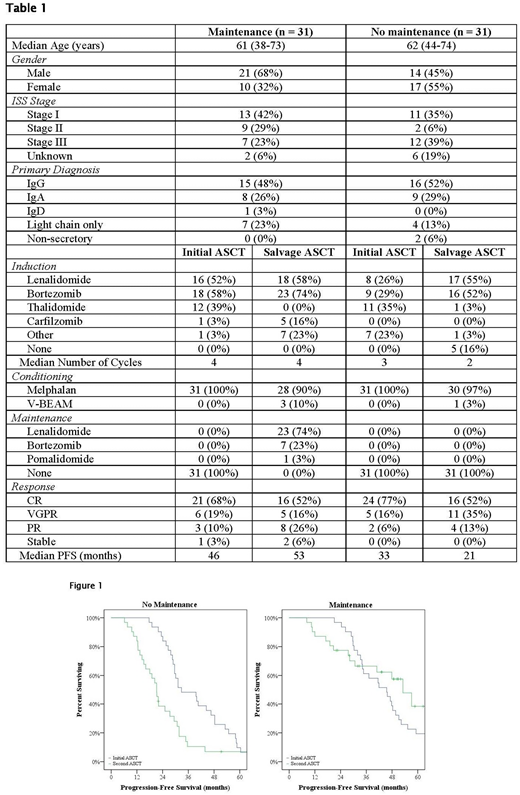
The maintenance cohort consisted of 31 patients, with 68% (n = 21) males and 32% (n = 10) females; the median age at salvage ASCT was 61 years (range 38-73). The no-maintenance cohort consisted of 31 patients as well with 45% (n = 14) males and 55% (n = 17) females. Their median age at salvage ASCT was 62 years (range 44-74). The characteristics of the two cohorts are summarized in Table 1.
Most patients received PIs and/or IMIDs as part of their induction regimens prior to initial ASCT. All received melphalan conditioning. The response to treatment was similar between the two cohorts, with respective CR rates of 68% (n = 21) and 77% (n = 24) and median progression-free survival (PFS) of 46 months compared to 33 months.
Following relapse, 16% (n = 5) of patients in the no-maintenance cohort proceeded directly to salvage ASCT without re-induction. All other patients received re-induction, mostly with PIs and/or IMIDs, with a median of 4 cycles for the maintenance cohort and 2 cycles for the no-maintenance cohort. For conditioning prior to salvage ASCT, 4 patients received Velcade-BEAM conditioning as part of a prospective trial at our site (NCT01653418); 3 from the maintenance cohort and 1 from the no-maintenance cohort. The rest received melphalan conditioning. Both cohorts had a CR rate of 52% (n = 16) post-salvage ASCT.
Maintenance therapy after salvage ASCT consisted of lenalidomide (74%, n = 23), bortezomib (23%, n = 7), or pomalidomide (3%, n = 1). Three of the patients on bortezomib were originally started on lenalidomide but were switched due to intolerance.
At time of data collection, the median follow-up was 49 months (range 9-105) for the maintenance cohort and 61 months (range 19-113) for the no-maintenance cohort. 45% (n = 14) of patients in the maintenance cohort and 90% (n = 28) of the no-maintenance cohort had relapsed.
In the maintenance cohort, PFS following salvage ASCT was similar to what was observed following initial ASCT. The median estimated PFS post-salvage ASCT was 53 months (95% CI 42-64) compared to 46 months post initial ASCT (p = 0.144). Conversely, in the no-maintenance cohort PFS following salvage was only about 60% that of initial ASCT (21 months [95% CI 18-24]; compared to 33 months; p = 0.002).
Conclusion: These results suggest that maintenance following salvage ASCT is associated with improved outcomes. Although patients who received maintenance post-initial ASCT were excluded, the benefits of maintenance post-salvage ASCT may extend to them as well. Ongoing prospective clinical trials will further clarify these benefits.
Schroeder:Amgen Inc.: Consultancy, Membership on an entity's Board of Directors or advisory committees. Wildes:Janssen: Research Funding. Vij:Jazz Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Jansson: Honoraria, Membership on an entity's Board of Directors or advisory committees; Karyopharma: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal